
The Shift from DSM-IV to DSM-5: A Pivotal Moment
When the American Psychiatric Association released the DSM-5 in 2013, it made significant changes to how PTSD is defined and diagnosed. These weren’t minor tweaks. The new criteria fundamentally altered which trauma survivors receive a diagnosis, how their symptoms are understood, and which treatments clinicians recommend. Understanding these changes helps you recognise why your own experience may be framed differently by different mental health professionals.
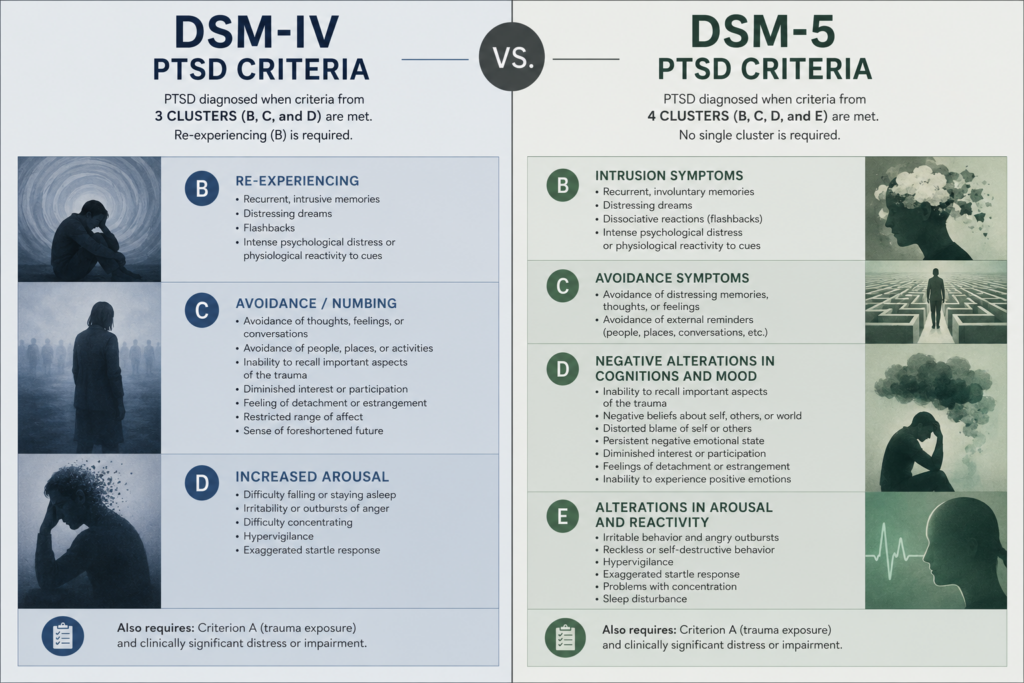
The DSM-IV (published in 1994) defined PTSD using four clusters: re-experiencing, avoidance, numbing, and hyperarousal. Sounds straightforward, but clinicians found real gaps. Some people with clear trauma responses didn’t fit neatly into those categories. Others were diagnosed when their symptoms seemed less severe than they actually were. The DSM-5 restructured everything.
What the DSM-5 Added: Two New Symptom Clusters
The DSM-5 expanded PTSD from four clusters to four more granular ones. The most significant addition was the negative alterations in cognition and mood cluster. This recognises that trauma doesn’t just make you afraid or avoidant. It can fundamentally change how you think about yourself, others, and the world. Persistent negative beliefs (“I am broken”, “no one can be trusted”, “the world is entirely dangerous”) now count as core PTSD symptoms in their own right.
The second major restructuring separated changes in arousal and reactivity into its own distinct cluster. This acknowledges that hypervigilance, irritability, reckless behaviour, and sleep disturbance form a coherent group of trauma responses that deserve specific clinical attention.
A third cluster focuses on intrusive symptoms (what survivors experience when trauma memories break through unexpectedly). The fourth addresses avoidance, now defined more narrowly than before. This precision matters because it means clinicians can identify which specific symptom patterns you’re experiencing and tailor interventions accordingly.
What Changed About Diagnosis Itself
Under DSM-IV rules, you needed symptoms from all four clusters to qualify for a diagnosis. The DSM-5 requires symptoms from all four new clusters, but the threshold is different. You need at least one intrusive symptom, one avoidance symptom, two negative cognition/mood symptoms, and two arousal/reactivity symptoms. This sounds more permissive, but the reality is more nuanced. Some people who would have been diagnosed under DSM-IV criteria no longer qualify, whilst others who were missed now receive recognition.
The DSM-5 also extended the diagnostic window. Previously, symptoms had to emerge within three months of trauma. Now, delayed-onset PTSD (where symptoms first appear months or even years later) is formally recognised. This reflects clinical reality: trauma can lie dormant, then surface when triggered by life circumstances, anniversary dates, or new traumas.
Why These Changes Matter for Treatment
The expanded definition of negative cognition and mood symptoms has reshaped trauma treatment. Cognitive processing therapy and trauma-focused cognitive behavioural therapy now explicitly target maladaptive beliefs about safety, control, and self-worth. Research on cognitive processing therapy shows that addressing these negative beliefs directly improves outcomes more effectively than earlier approaches that focused primarily on fear reduction.
The clearer separation of arousal symptoms has also driven development of treatments specifically targeting sleep, irritability, and reckless behaviour. Rather than lumping all these responses together as “hyperarousal”, clinicians now recognise they may require different interventions. Someone struggling with sleep might benefit from different strategies than someone whose primary issue is emotional reactivity.
The Controversy: Did the DSM-5 Get It Right?
Not everyone agrees the changes improve diagnosis. Some researchers argue the new criteria cast too wide a net, potentially over-diagnosing PTSD in people with significant distress but not necessarily trauma-specific pathology. Others contend the criteria still miss complex presentations, particularly in people with PTSD from violent childhood trauma, where symptoms may look quite different from those following single-incident adult trauma.
The DSM-5 also removed the requirement that trauma be “outside the range of normal human experience”, replacing it with an objective exposure criterion (direct experience, witnessing, learning about it happening to someone close, or repeated exposure to details). This shift recognises that subjective impact matters less than the type of event itself. Some clinicians see this as more objective. Others worry it misses people who experience profound trauma responses to events that don’t meet the strict exposure definition.
What This Means for Your Diagnosis
If you’ve been diagnosed with PTSD under DSM-5 criteria, your diagnosis reflects a more refined understanding of trauma’s impact than earlier frameworks allowed. Your symptoms are being mapped onto a more specific set of categories, which should theoretically lead to more targeted treatment. However, if you’ve been told you don’t meet criteria, it’s worth exploring whether a clinician familiar with complex or delayed presentations might see things differently.
Current research continues to refine how PTSD is understood, and future diagnostic manuals will likely evolve further. The DSM-5 represented a significant step forward in recognising the diversity of trauma responses, but it’s not the final word. Understanding why the criteria changed helps you engage more critically with your own diagnosis and advocate for the treatment approach that actually fits your experience.




